











Reducing Mortality Through Earlier Sepsis Intervention

- 120 lives saved.
- 50 percent relative reduction in mortality for patients with emergency department (ED) present on admission (POA) severe sepsis.
- 14 percent relative reduction in mortality for patients with ED POA septic shock.
- $5.5 million in savings, the result of reducing average variable cost of care for ED POA and inpatient cohort with sepsis, while also capturing patients for downstream care delivery.
Community Health Network had implemented evidence-based care; however, the sepsis mortality rate remained higher than desired. To address this situation, the health system established a sepsis council to coordinate a sepsis improvement plan and implemented an analytics platform to gain insight into sepsis care performance.
SEPSIS: A COSTLY DISEASE STATE WITH HIGH MORTALITY
Sepsis ranks highest among admissions for all disease states, accounting for more than $24 billion in annual hospital expenses. Up to 80 percent of ED patients present with it upon admission, and it is related to one-third of all hospital deaths.1,2
A non-profit healthcare organization serving central Indiana, CHNw is consistently ranked among the nation’s most integrated healthcare systems. Based in Indianapolis, CHNw serves more than 539,000 patients and employs over 15,000 caregivers. It delivers exceptional healthcare services, where and when patients need them—in hospitals, health pavilions, and doctor’s offices, as well as workplaces, schools, and homes. CHNw values patients first and is committed to providing patient-centered care and outstanding service, delivered with respect and compassion.
ADDRESSING SEPSIS REQUIRES STANDARDIZED PRACTICES
CHNw had implemented evidence-based sepsis care; however, the mortality rate remained higher than desired. A standard process was required for early identification of patients with sepsis. Once sepsis was identified, there was no consistent mechanism to notify providers that the patient had sepsis, delaying diagnostic testing and treatment. The organization observed unintended variation in ED sepsis care across its four campuses.
Further hampering efforts, CHNw lacked actionable data that could be used to provide insight into performance on the timeliness of key sepsis care interventions. The organization needed a comprehensive data-driven approach for early notification of possible sepsis, and to decrease unwarranted variation to drive down sepsis mortality and cost of care.
REDUCING SEPSIS MORTALITY THROUGH DATA-DRIVEN APPROACH
To improve sepsis care and outcomes, CHNw established a sepsis council—an interdisciplinary team including physicians involved in the care of patients with sepsis, registered nurses, program managers, informaticists, data analysts, financial analysts, clinical nurse specialists, and nursing leadership—and engaged the council in developing and implementing a sepsis improvement plan.
To help guide the sepsis council’s efforts, CHNw utilized the Health Catalyst® Data Operating System (DOS™) and a robust suite of analytics applications, including the Sepsis Analytics Accelerator to gain insight into sepsis care performance. Data from this platform informed CHNw that 75 percent of its patients arrived into the emergency department with sepsis. CHNw prioritized patients in the ED with sepsis POA, specifically patients with severe sepsis and septic shock, for improvement.
After reviewing the available literature and best practices, the sepsis council focused its efforts on engaging frontline staff in improving the speed of sepsis recognition and treatment, and the timeliness of antibiotic administration.
To improve reliability and reduce unwarranted sepsis care variation, CHNw incorporated evidence-based order sets for sepsis care into the EMR. These order sets were optimized to align with the ED provider workflow, and aligned with the order sets used most often by ED providers. They are also designed to meet evidence-based, three-hour sepsis bundle components, including:
- Procuring a lactate level.
- Obtaining blood cultures prior to administration of antibiotics.
- Administering a broad-spectrum antibiotic.
- Dispensing intravenous fluid bolus if the patient’s systolic blood pressure is below 90.
CHNw provided its interdisciplinary team education to improve the recognition of sepsis signs and symptoms, including the need to “think sepsis” when patients present with vague symptoms such as lethargy, changed mental status, confusion, decreased urinary elimination, and general risks for infection.
To support the team in the prompt identification of sepsis, CHNw implemented a sepsis alert, using the systemic inflammatory response syndrome (SIRS) criteria to prompt the care team to “think sepsis.” When this condition is suspected, the ED registered nurse broadcasts a “team activate” which brings the physician to the bedside. If the physician’s clinical assessment determines the patient meets criteria, then the physician activates the “code sepsis.” This code alerts the larger care team that there is a patient suspected with sepsis, helps get the physician to the bedside of that patient faster, and notifies the pharmacy that there may be a need for additional medications. CHNw also now stocks the most commonly used antibiotics in the ED, ensuring they are readily available to be administered in a timely manner.
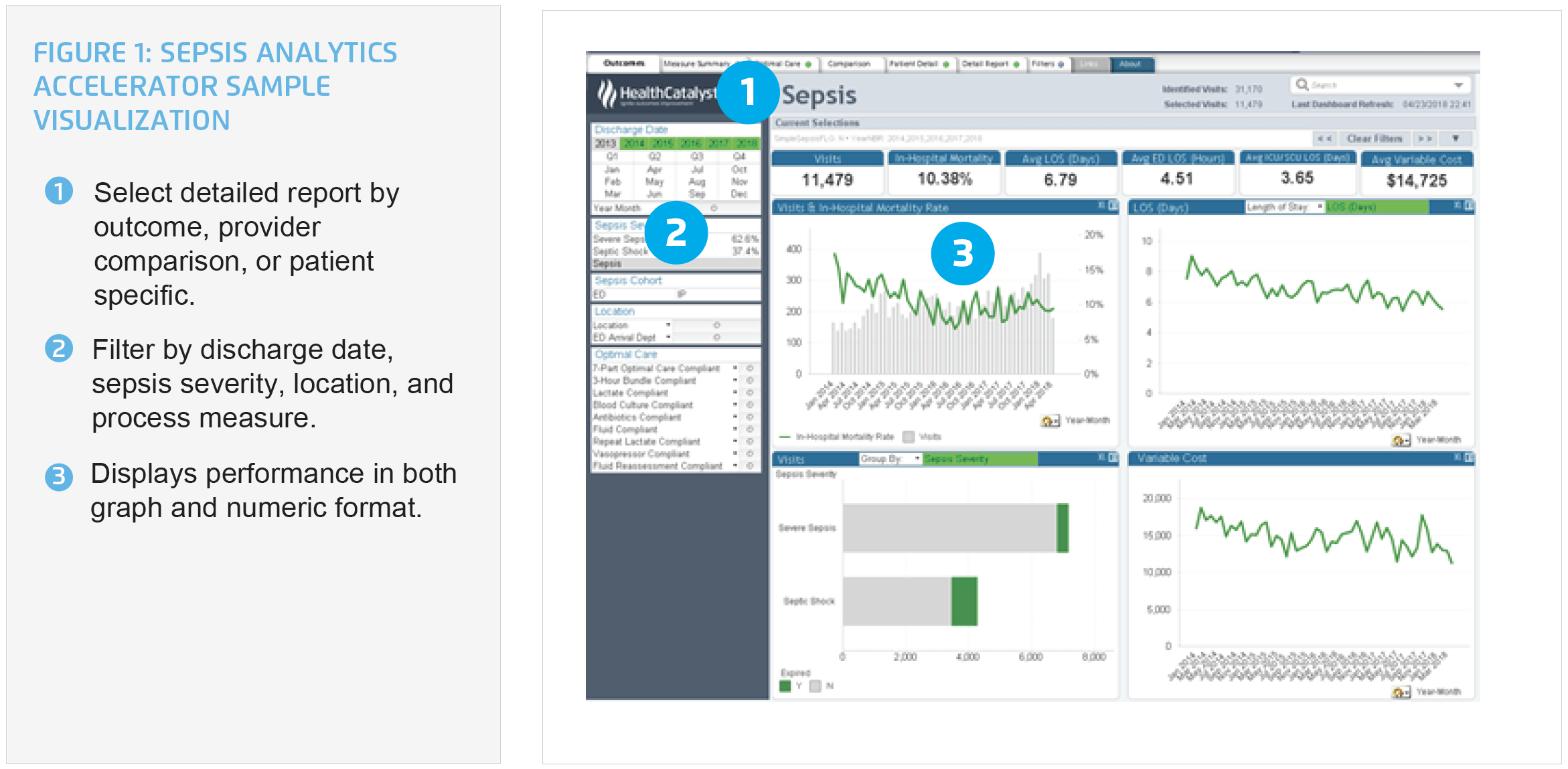
CHNw leverages the analytics accelerator to monitor performance for process measures, including the timely administration of antibiotics, and evaluates the impact on patient outcomes and financial performance. Using the analytics accelerator, CHNw can easily and effectively monitor the number of visits for patients with sepsis, mortality rates, length of stay (LOS), average variable cost, adherence to process measures, including the timely administration of antibiotics, and patient-level details (see Figure 1).
The sepsis council, program managers, and leaders use data from the analytics accelerator to monitor performance, providing feedback to physicians and nursing staff about their performance, clearly linking the impact of their interventions to patient outcomes.
In addition to using the analytics application to facilitate data-driven improvement, CHNw has developed a model for comprehensive financial analysis. The organization can evaluate detailed cost data and is able to better understand why costs are higher in one population. For patients with sepsis, CHNw evaluates the ED workflow, respiratory care costs, cost difference by discharge location, average LOS, case mix index, and the impact of seasonality on costs and outcomes.
CHNw can use the comprehensive financial data to calculate cost savings associated with its sepsis improvement work.
RESULTS
CHNw’s data-driven sepsis improvement efforts have improved the consistency of care provided to its patients, and positively impacted clinical and financial outcomes, including:
- 48 percent relative reduction in mortality for patients with ED POA sepsis – 66 lives saved.
- 40 percent relative improvement in the timeliness of door to antibiotic administration for ED POA sepsis.
- More than doubled three-hour bundle compliance for ED POA sepsis.
- 50 percent relative reduction in mortality for patients with ED POA severe sepsis – 34 lives saved.
- 51 percent relative improvement in the timeliness of door to antibiotic administration for ED POA severe sepsis.
- 65 percent relative improvement in three-hour bundle compliance for ED POA severe sepsis.
- 14 percent relative reduction in mortality for patients with ED POA septic shock – 20 lives saved.
- 38 percent relative improvement in the timeliness of door to antibiotic administration for ED POA septic shock.
- More than doubled three-hour bundle compliance for ED POA septic shock.
- $5.5 million in savings, the result of reducing average variable cost of care for ED POA and inpatient cohort with sepsis, while also capturing patients for downstream care delivery.
As a result of its work to determine the financial benefit of its sepsis improvement efforts, CHNw has developed a model for financial analysis that can be spread throughout the organization.“We integrated sepsis best practices with the nurses’ workflow to ensure patients get the care they need in the emergency department.”
– Dawn Sullivan-Wright, Clinical Nurse Specialist, Emergency Services
WHAT’S NEXT
CHNw remains committed to further reducing sepsis mortality rates. The health system plans to expand its sepsis improvement, focusing on timely recognition and treatment of inpatients with potential sepsis.
REFERENCES
- Center for Disease Control and Prevention. (2018). Making health care safer Think sepsis. Think about time.
- Joo, Y. M., Chae, M. K., Hwang, S. Y., Jin, S., Lee, T. R., Cha, W. C., Jo, I. J., … Shin, T.G. (2014). Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department. Clinical Experience Emergency Medicine, 1(1), 35-40.
This website stores data such as cookies to enable essential site functionality, as well as marketing, personalization, and analytics. By remaining on this website you indicate your consent. For more information please visit our Privacy Policy.