











Enhancing Mental Health Care Transitions Reduces Unnecessary Costly Readmissions

- 27 percent relative reduction in potentially preventable readmission rate.
- 80 percent patient retention rate in established outpatient mental health services.
Nationally, hospitalization for persons with mental health disorders has increased faster than hospitalization for any other condition. Of concern is the lack of bed space to intake these patients on a timely basis. In Minnesota, for example, more than 50 percent of available state psychiatric beds were closed between 2005 and 2010. Furthermore, readmission rates for patients with mood disorders is higher than any other mental health condition, with 15 percent readmitted within 30 days of hospital discharge and up to 22.4 percent of patients with schizophrenia being readmitted. While the average cost of a readmission in the U.S. is approximately $7,200, of greater concern is hospital readmission represents poor patient outcomes related to lack of adequate access to community mental health resources and challenges with adherence to care plans needed to prevent chronic relapse.
In response to these challenges, Allina Health put a new care transition process in place, redesigned workflow, and added key patient support roles. To measure the effectiveness of new interventions, Allina relied on the Health Catalyst Analytics Platform, which includes the Late-Binding™ Enterprise Data Warehouse and a broad suite of analytics applications.
HIGHER READMISSION RATES FOR PATIENTS WITH MENTAL HEALTH ISSUES
Nationally, hundreds of thousands of people in need of mental health care seek help from local hospitals. In 2012, inpatient admissions for mood disorders reached 847,000, with inpatient stays for schizophrenia, one of the most acute mental illnesses, reaching 383,000. In 2011, it was estimated that 37 percent of individuals with disabilities and on Medicare had a serious mental disorder.1
Both mood disorders and schizophrenia are associated with relatively high readmission rates, further taxing the already limited availability of inpatient mental health treatment. Within 30 days, 15 percent of patients with mood disorders are readmitted nationally, while 22.4 percent of patients with schizophrenia are readmitted. Across the U.S., the average cost for the repeated hospital stay is approximately $7,200.2 Key factors influencing the rate of readmission include issues with medication management, poor outpatient follow-up and/or treatment, and comorbid substance use disorders.3,4
Allina Health, an integrated delivery system in Minnesota, provides inpatient and outpatient mental health care to communities throughout Minnesota and western Wisconsin. Recognizing that patients with mood and mental health disorders are particularly vulnerable to readmission, Allina committed to improving outcomes for mental health patients.
STRETCHED RESOURCES PREVENT PATIENTS FROM RECEIVING CONTINUED TREATMENT
At Allina, mental health patient acuities have been worsening, while inpatient and outpatient services are stretched ever thinner. Statewide in Minnesota, between 2005 and 2010 more than 50 percent of available state psychiatric beds were closed. Moreover, Minnesota has fewer psychiatrists than any other state and access to outpatient resources like crisis stabilization and rehabilitation services is increasingly more challenging.
This lack of sufficient inpatient and outpatient mental health services has resulted in an influx of patients coming to the emergency department (ED) to receive mental health care, with many boarded in the ED for extended periods of time while they wait for an available inpatient bed or outpatient service. Post discharge, many patients have no contact with their outpatient mental health provider until weeks or months after discharge. Establishing case management services for patients with complex mental health needs can take up to 60 or even 90 days as the referrals for services make their way through the approval process.
With these challenges as the backdrop, Allina Health was determined to improve outcomes for patients with mental illness, including reducing their rate of readmission and improving their access to community supports. Abbott Northwestern Hospital (ANW), part of Allina Health, embarked on a mission to maximize the effectiveness of care planning in the inpatient mental health units and ensure both a smooth transition and successful treatment in the outpatient setting.
ENHANCING MENTAL HEALTH CARE TRANSITIONS
To achieve the above objectives, Allina knew it would need to enhance partnerships with other organizations in the community while introducing new roles and interventions internally. The latter would require a redesign in workflow, aided by data and analytics to evaluate the effectiveness of new measures.
Piloting a new transition process. Allina received a grant to pilot an enhanced care transitions project at ANW in partnership with the Minnesota Community Healthcare Network (MCHN), supporting patients from seven different counties.
MCHN includes five outpatient mental health agencies that provide for an integrated healthcare approach and comprehensive treatment for individuals living with serious, persistent mental illness and other complex conditions, such as chemical dependency, chronic health conditions, and socioeconomic challenges.
The aim of the project was to increase access to community support for ANW adult mental health inpatients at the highest risk for readmission by developing and implementing a collaborative discharge and transition pilot. A primary goal of the project was to reduce readmissions by at least 10 percent. To support this goal, the team worked to:
- Develop mental health interventions that enhance chances of successful recovery in the outpatient setting and subsequently reduce readmissions.
- Improve access to community mental health resources while a patient is still hospitalized.
- Create a patient-centered recovery model that promotes early patient and family engagement in discharge planning.
- Improve patient advocacy in treatment and demonstrate improvements in patient experience.
- Improve communication between inpatient and outpatient resources to ensure best care transitions and follow-up.
In addition to monitoring process measures related to the recovery plan and outreach, the readmission rate was established as the key performance indicator.
Optimizing the EHR for better documentation and analytics. Allina revised its EHR to support documentation of community care coordination, transition meetings, follow-up appointments, transmission of discharge records, and goal setting meetings with the patient and families.
Allina then utilized the Health Catalyst Analytics Platform, which includes the Late-Binding™ Enterprise Data Warehouse and broad suite of analytics applications, to aggregate data from the EHR. Using the platform, Allina can monitor and evaluate both process of care and outcome measures.
Engaging patients and building trust. Allina introduced two new roles at ANW that have been instrumental in supporting a successful transition and activation of outpatient resources: a mental health navigator and a peer support specialist.
The mental health navigator is a mental health professional who partners directly with the patient and care team to establish essential outpatient services, enhance discharge planning, support patient-centered recovery initiatives, and conduct routine outpatient follow-up with MCHN contacts and patients.
The peer support specialist is an individual with a mental health diagnosis who has been in recovery for a minimum of one year and has completed peer support specialist certification. As the patient’s advocate, the peer support specialist fosters a trusting relationship with the patient, participates in or runs recovery groups, encourages patients to engage and participate more deeply in care planning, and provides outpatient follow-up to maintain recovery and prevent crisis as needed.
Proactive patient engagement. With these new roles in place, Allina redesigned the inpatient workflow. Following admission, the social worker completes a diagnostic assessment, and the mental health navigator reviews every adult patient to identify if they meet inclusion criteria for the pilot. Pilot inclusion critieria includes the following: lives in the metro area; has a diagnosis with a high risk of readmission; was previously hospitalized or visited the emergency department for mental health concerns, and lacks available outpatient services. If the patient meets these criteria, the mental health navigator invites the patient to participate in the program. If the patient declines, the peer support specialist is engaged to meet with the patient and help encourage participation in the program. Very few patients declined participation in the program throughout the course of the pilot.
Patients who agree to participate in the program sign a release of information form that lasts for five years from the date of signature, allowing easy and ongoing bilateral exchange of patient information between Allina and the five participating MCHN agencies. This ensures that communication between the mental health experts at the hospital and in the in the community does not end when the patient is discharged from the hospital.
Effective care coordination. Unique patient needs are identified by the mental health navigator and referrals to community services are sent to the MCHN community hub via a service request. The MCHN community coordinator reviews the service request and shares it with the five outpatient mental health agencies. The MCHN agencies review the patient’s needs and respond within 4-6 hours or faster with the resources they are able to provide. The mental health navigator reviews the options with the patient and together with the MCHN community coordinator identifies which agency is best able to meet the patient’s needs.
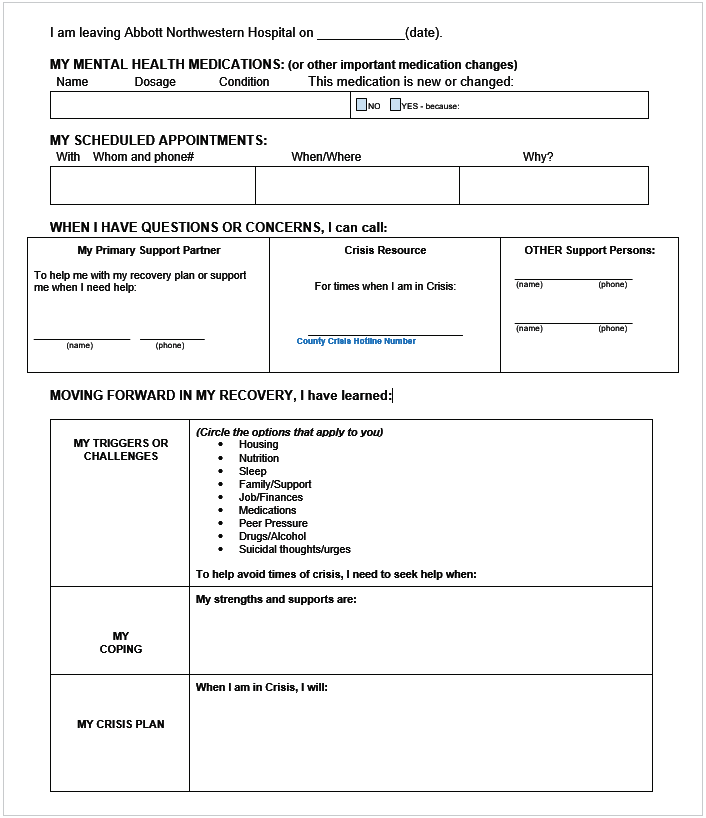
Prior to discharge, some key actions take place. Firstly, the selected MCHN agency is contacted to initiate an onsite assessment and to establish a proactive outpatient plan while the patient is still hospitalized. This early engagement helps bypass delays in establishing timely and effective outpatient care and enhances relationship building that increases likelihood for continued patient participation in services once discharged. For many patients, the MCHN contacts will come onsite for multiple visits with the patients, especially if their care is highly complex. Secondly, prescriptions needed after discharge are filled at the hospital to increase chances of medication adherence in the outpatient setting. Pharmacy educators offer group education opportunities to review the importance of medications, review potential side effects, and answer any patient questions. Thirdly, the patient participates in transition meetings, plans for discharge, establishing goals, and their recovery plan. The Recovery Plan is developed with the patient early in admission process and is written in patient-centered, easy to understand language (see Figure 1).
Upon discharge, records regarding the patient’s inpatient stay and discharge needs are sent to the next level of care within 24 hours. The MCHN agency contacts the patient no later than 48 hours after discharge, and in many cases, will make immediate contact or even come to the hospital to visit with the patient on day of discharge.
Both the mental health navigator and the peer support specialist follow-up after discharge. A follow-up phone call is set up with the MCHN agency contact and the patient between 30-45 days post-discharge to review recovery status and help identify opportunities to improve outpatient care.
A team approach keeps patients out of crisis. Should challenges arise while the patient is receiving care in the outpatient setting, the MCHN agencies can contact the mental health navigator and mental health experts at ANW for assistance.
In one compelling example, a patient receiving care in the outpatient setting was robbed, and the patient’s medications were stolen. Since the prescription had already been filled within a 30-day period, insurance would not cover the cost of a refill. The MCHN agency contacted the mental health navigator, who subsequently collaborated with the inpatient mental health prescribers and pharmacy staff. Ultimately, the team contacted the insurance company and were successful in getting coverage for the refills. This ensured the patient could take their medication as prescribed, avoiding an unnecessary readmission.
Another patient was discharged to a chemical dependency treatment program. Unfortunately, she was exited from the program, which meant she was no longer compliant with the terms of her probation and was at risk of being jailed. The patient reached out to the navigator, who helped the patient find a crisis residence, maintaining compliance with her terms of probation and keeping her out of jail.
In yet another example, a 22-year-old man who was homeless had been admitted multiple times for chemical dependency and a suicide attempt. He began working with the peer specialist and was discharged to a chemical dependency treatment facility for a one-year outpatient treatment. It was important to the patient to be admitted to a faith-based treatment facility, which the team supported him in doing. The peer specialist met with the patient frequently, establishing a relationship and supporting the patient in his recovery. Today, the patient is working to become a peer support specialist, completing the training that will allow him to help others facing similar challenges in the future.
RESULTS
The enhanced care transitions program at Allina is improving care transitions for patients, and decreasing mental health readmission rates.
- 27 percent relative reduction in potentially preventable readmission rate. When compared to a control group, those who received enhanced care transitions had a much lower rate of readmission. Nationally, the 30-day readmission rate for patients with mood disorders is 15 percent. The 30-day readmission rate for patients with schizophrenia is 22.4 percent. The enhanced care transitions program is achieving a readmission rate far below the national average, with only 4.6 percent of the enhanced care transitions program patients readmitted within 30 days.
- 97 percent relative improvement in the transmission of records within 24 hours of discharge.
- Multiple processes of care improved.
- 95 percent of patients have a recovery plan.
- 90 percent of patients are successfully established with a MCHN agency before discharge.
- 88 percent of patients receive a MCHN agency onsite visit prior to discharge. If an onsite visit was not possible due to fast discharge timelines, all efforts to have a conference call with the patient was made.
- 94 percent of patients have a follow-up appointment prior to discharge.
- 100 percent of patients receive a closed-loop call within 45 days of discharge.
- 92 percent of patients successfully arrived at their follow-up appointment.
- Two patients were incarcerated, and unable to go to their follow-up appointment. One patient preferred a different psychiatrist and was subsequently rescheduled.
- More than 80 percent patient retention. Importantly, the enhanced care transitions program is successfully retaining over 80 percent of patients in the established outpatient services at 30-days post-discharge, far surpassing national retention rates.
“Tracking key outcome metrics really show us what we’re successful at so we can modify our interventions and the program design.”
– Heather Sievers
Performance Improvement Advisor
WHAT’S NEXT
Allina has created a blueprint for other provider organizations to study to solve the problems that hinder some of our most vulnerable patients from receiving the compassionate care they deserve. Having demonstrated success and identified more patients who could benefit from the enhanced care transitions program, Allina is working to secure the funding required for program expansion.
REFERENCES
1, 2, 3. Heslin, K. C. & Weiss, A. J. (2015). Hospital readmissions involving psychiatric disorders, 2012, HCUP statistical brief #189. Agency for Healthcare Research and Quality.
4. Finnerty, M. (2012, June 21). The quality concern: Behavioral health inpatient readmissions.
ABOUT HEALTH CATALYST
Health Catalyst is a next-generation data, analytics, and decision support company committed to being a catalyst for massive, sustained improvements in healthcare outcomes. We are the leaders in a new era of advanced predictive analytics for population health and value-based care. With a suite of machine learning-driven solutions, decades of outcomes-improvement expertise, and an unparalleled ability to integrate data from across the healthcare ecosystem. Our proven data warehousing and analytics platform helps improve quality, add efficiency and lower costs in support of more than 85 million patients and growing, ranging from the largest US health system to forward-thinking physician practices. Our technology and professional services can help you keep patients engaged and healthy in their homes and workplaces, and we can help you optimize care delivery to those patients when it becomes necessary. We are grateful to be recognized by Fortune, Gallup, Glassdoor, Modern Healthcare and a host of others as a Best Place to Work in technology and healthcare.
Visit www.healthcatalyst.com, and follow us on Twitter, LinkedIn, and Facebook.
This website stores data such as cookies to enable essential site functionality, as well as marketing, personalization, and analytics. By remaining on this website you indicate your consent. For more information please visit our Privacy Policy.